Business Context
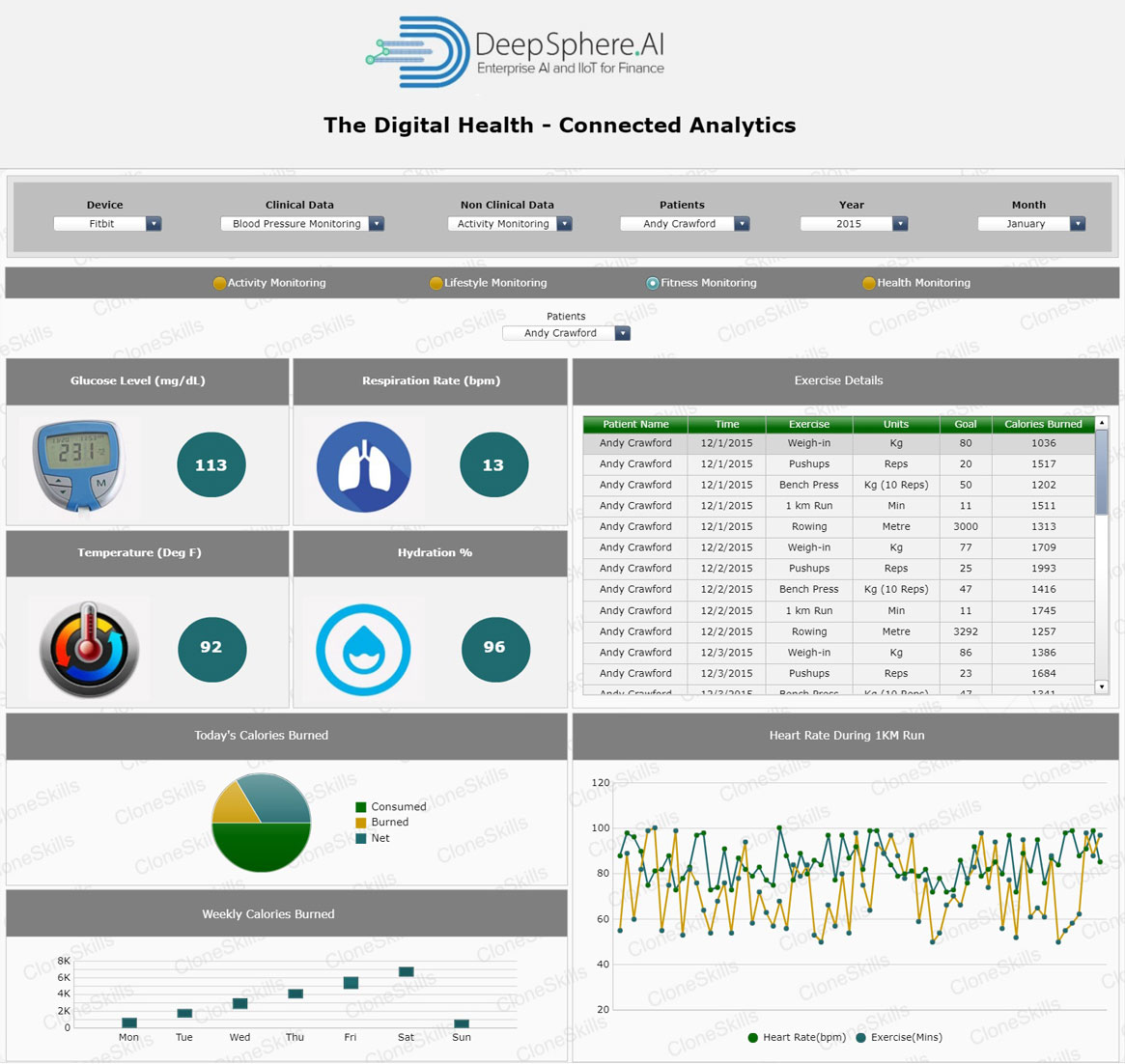
Fitness Monitoring is the measurement of glucose level, respiration, heart, and hydration rate. The blood “Glucose Level” is the amount of glucose in the blood. Glucose is a sugar that comes from the foods one eats. It is formed and stored inside the body. Glucose is the main source of energy for the cells in the body, carried through the cells in the bloodstream. One needs to keep blood sugar levels within a safe range to reduce the risk of diabetes and heart disease.
Respiratory Rate (RR) is the number of breaths one takes per minute. The normal respiration rate for an adult at rest is 12 to 20 breaths per minute. A respiratory rate that is under 12 breaths per minute or over 25 breaths per minute while resting is abnormal. Asthma, anxiety, pneumonia, congestive heart failure, narcotics, or drug overdose are conditions that can change respiration. Activity levels influence the respiration rate.
Heart Rate is the number of contractions (beats) of the heart per minute (bpm). The heart rate can vary according to the body's physical needs, including the need to absorb oxygen and excrete carbon dioxide. It is usually equal or close to the pulse measured at any peripheral point. Activities that can provoke change include physical exercise, sleep, anxiety, stress, illness, and the ingestion of drugs.
Hydration is the introduction of additional fluid into the body. Hydration sometimes helps to reduce the concentration of toxic substances in the tissues. Hydration Rate is the measure of fluids introduced in the body.
Model Details
- ElasticNet Regression
- Polynomial Regression
- Linear Regression
- Artificial Neural Networks